It's amazing how, the more QAnon's ludicrous conspiracy theories are debunked, the more risible they became in trying to justify them, like toddlers caught with their hands in the cookie jar, rather than admit the game's up and they've been rumbled.
One example of how far into the stratosphere QAnon conspiracists have gone in the justification for opposing measures to mitigate the COVID-19 pandemic, which is about to achieved its millionth American death, on the grounds that it's all a plot, somehow linked to a Satanic, cannibalistic paedophile, deep state conspiracy run by Hillary Clinton, Barak Obama and the Pope, and including Bill Gates, Andrew Faucci and others, is the so-called 'explosive report' by medical quackticioner, Dr. Bryan Ardis.
His 'explosive' report which he revealed on the far right Stew Peters Show, is that the SARS-CoV-2 virus that causes COVID-19 is not a virus at all but a modified snake venom which is passed on deliberately in drinking water. Seriously!
Here is how he arrived at that conclusion, not by analysis of drinking water, or by subjecting samples of the virus to biochemical analysis, but by a form of logic of which any self-respecting toddler might be proud, until they grew up enough to cringe in embarrassment at their childish thinking.
There are two ways of looking at the latest findings concerning the long-term effects of severe COVID-19.
If you are a creationist, you could marvel at the inventive genius of any intelligent designer who could design such a thing as the SARS-CoV-2 virus that causes COVID-19 just to increase the suffering in the world
If you are a caring and compassionate person, you can appreciate how this findings makes it imperative that as many people as possible are vaccinated and boosted in order to reduce the likelihood of someone else catching the disease and to help make the pandemic a thing of the past.
The finding, by researchers from the University of Missouri School of Medicine and MU Health Care shows that there is a significantly increased risk of developing dementia following a case of COVID-29-induced pneumonia, severe enough to requiring hospitalization.
The risk of new onset dementia was more common in COVID-19 pneumonia patients over the age of 70 in our study.
The type of dementia seen in survivors of COVID-19 infection mainly affects memory, ability to perform everyday tasks and self-regulation. Language and awareness of time and location remained relatively preserved.
The findings suggest a role for screening for cognitive deficits among COVID-19 survivors. If there is evidence of impairment during screening and if the patient continues to report cognitive symptoms, a referral for comprehensive assessment may be necessary.
Professor Adnan I. Qureshi, MD.
Professor of clinical neurology
MU School of Medicine.
For the study, the researchers analysed the records of 1.4 billion medical encounters prior to July 31, 2021. They selected patients hospitalized with pneumonia for more than 24 hours. Among 10,403 patients with COVID-19 pneumonia, 312 (3%) developed new onset dementia after recovering, compared to 263 (2.5%) of the 10,403 patients with other types of pneumonia diagnosed with dementia. This represents a 20% increase in the risk of dementia following COVID-19 pneumonia.
The study was only of new onset dementia. The median time interval between infection and dementia diagnosis was 182 days for COVID-19 patients. The study only included new onset dementia associated with hospital admission during a short follow-up period. Dr Qureshi said a more detailed study, conducted over a longer time may help to determine the reasons why COVID-19 is linked to dementia.
The authors give more details in the abstract to their open access paper published in the journal Open Forum Infectious Diseases:
Abstract
Background
Case series without control groups suggest that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection may result in cognitive deficits and dementia in the postinfectious period.
Methods
Adult pneumonia patients with SARS-CoV-2 infection (index hospitalization) and age-, gender-, and race/ethnicity-matched contemporary control pneumonia patients without SARS-CoV-2 infection were identified from 110 healthcare facilities in United States. The risk of new diagnosis of dementia following >30 days after the index hospitalization event without any previous history of dementia was identified using logistic regression analysis to adjust for potential confounders.
Results
Among 10 403 patients with pneumonia associated with SARS-CoV-2 infection, 312 patients (3% [95% confidence interval {CI}, 2.7%–3.4%]) developed new-onset dementia over a median period of 182 days (quartile 1 = 113 days, quartile 3 = 277 days). After adjustment for age, gender, race/ethnicity, hypertension, diabetes mellitus, hyperlipidemia, nicotine dependence/tobacco use, alcohol use/abuse, atrial fibrillation, previous stroke, and congestive heart failure, the risk of new-onset dementia was significantly higher with pneumonia associated with SARS-CoV-2 infection compared with pneumonia unrelated to SARS-CoV-2 infection (odds ratio [OR], 1.3 [95% CI, 1.1–1.5]). The association remained significant after further adjustment for occurrence of stroke, septic shock, and intubation/mechanical ventilation during index hospitalization (OR, 1.3 [95% CI, 1.1–1.5]).
Conclusions
Approximately 3% of patients with pneumonia associated with SARS-CoV-2 infection developed new-onset dementia, which was significantly higher than the rate seen with other pneumonias.
The findings from this study, with the findings in the study which was the subject of my last blog post which showed the efficacy of the vaccines in children, give a very clear message to anyone with a sense of social responsibility, which I appreciate tends not to include evangelical creationists and members of extremist right-wing antivaxxer cults, is that vaccinations work and should be encouraged, if we are ever to put an end to this pandemic and to reduce the suffering it has wrecked worldwide.
Probably what evangelical creationists hate most about the vaccines is that they represent a considerable triumph of science over what they believe to be the creation of their god, visited on mankind for disagreeing with evangelical creationists.
Don't be a Covidiot!
Get vaccinated or get boosted, Now!
A new study has shown that the Pfizer-BioNTech mRNA COVID-19 vaccine significantly reduces the proportion of sever COVID-19 infections, reducing the risk of hospitalisation in 5–11-year-olds by two-thirds. Although it was lower for the Omicron variant than for Delta, protection against hospitalisation remained high for 12–18-year-olds. It also gave high protection against critical COVID-19 requiring life-supporting interventions for adults during both Delta and Omicron waves.
A study by researchers at the University of Virginia, Charlottesville, VA, USA, has shown why it is not only important to get vaccinated, but why it is just as important to get boosted and this is especially true for those vaccinated with Pfizer's BNT162b2 vaccine, but also for those vaccinated with either Moderna's mRNA-1273 vaccine or the single-shot Johnson & Johnson Ad26.COV2.S vaccine.
It shows that for the Pfizer vaccine, antibody levels rose more slowly than with the Moderna mRNA vaccine and fall more quickly, especially in older people. Antibody levels also fell with the Moderna vaccine, but age did not appear to make a significant difference. Peak levels were reached after about 20 days for all three vaccines, but levels for Pfizer and Moderna were some 50 times higher than with Johnson & Johnson's Ad26.COV2.S vaccine.
According to the University of Virginia news item:
Yet more evidence, if any were needed, of the efficacy and desirability of getting vaccinated against COVID-19 was provided today in a paper published by a Swiss team from the Université de Genève (UNIGE) and the Hôpitaux universitaires de Genève (HUG). The results of their study were published in Nature Medicine a few days ago.
The team have shown that vaccinations reduce the viral load and thus the infectivity of vaccinated people who are unfortunate to become infected.
The press release from the Université de Genève explains:
This heat map reveals significant differences in the amounts of fertility-related proteins in the semen of healthy men (control) and those who had recovered from COVID-19 (COVID-19R).
With the SARS-CoV-2 pandemic far from over, new research shows why men should get vaccinated to avoid the risk of an infection seriously affecting their fertility.
The research by Indian scientists working at the Department of Biosciences and Bioengineering at the Indian Institute of Technology in Mumbai, has shown that even a mild or moderate illness could change the levels of semen proteins related to male reproductive function.
The information supplied by the Americam Chemical Society (ACS) explains more:
Many people who recover from COVID-19 experience long-term symptoms, such as brain fog or heart problems. Increasing evidence suggests that the virus can also impair fertility. Now, researchers reporting in ACS Omega have analyzed protein levels in semen of men who have recovered from COVID-19. The pilot study suggests that even mild or moderate illness could change the levels of proteins related to male reproductive function, the researchers say.
Although SARS-CoV-2 mainly affects the respiratory system, the virus — and the body’s response to it — also damages other tissues. Recent evidence indicates that COVID-19 infection can reduce male fertility, and the virus has been detected in male reproductive organs. Firuza Parikh and Rajesh Parikh at Jaslok Hospital, Sanjeeva Srivastava at the Indian Institute of Technology and colleagues wondered if COVID-19 infection could have long-term impacts on the male reproductive system. To find out, they decided to compare levels of proteins in the semen of healthy men and those who previously had mild or moderate cases of COVID-19.
The researchers analyzed semen samples from 10 healthy men and 17 men who had recently recovered from COVID-19. None of the men, who ranged in age from 20 to 45, had a prior history of infertility. The team found that the recovered men had significantly reduced sperm count and motility, and fewer normally shaped sperm, than men who hadn’t had COVID-19. When the researchers analyzed semen proteins using liquid chromatography-tandem mass spectrometry, they found 27 proteins at higher levels and 21 proteins at lower levels in COVID-19-recovered men compared with the control group. Many of the proteins were involved in reproductive function. Two of the fertility-related proteins, semenogelin 1 and prosaposin, were present at less than half their levels in the semen of the COVID-19-recovered group than in the semen of controls. These findings suggest that SARS-CoV-2 has direct or indirect effects on male reproductive health that linger after recovery, the researchers say. The work might also reveal insights into the pathophysiology of human reproduction in recovered men, they add. However, they note that larger studies should be done to confirm these findings, and a control group of men who recently recovered from other flu-like illnesses should be included to ensure that the findings are specific for COVID-19.
The team's findings were published open access yesterday in AMC Omeg:
New Zealand’s Omicron wave may be peaking, but we’ll continue to record thousands of new cases each day and most people who test positive or are hospitalised with COVID will have been vaccinated.
This is exactly what we should expect and it’s no reason to doubt vaccine effectiveness.
The principal reason why a lot of COVID cases are vaccinated is because most New Zealanders are now vaccinated. As of today, about 94% of people 12 years and older have had two or more vaccine doses, and even if their risk of catching COVID is significantly lower than for an unvaccinated person, they vastly outnumber those who aren’t.
Omicron is not mild. The only reason it appears mild is because we have excellent vaccines. If we didn't have the high vaccine coverage we have in NZ, we would be in a truly dire situation right now https://t.co/0tvdIaNKdk
In the week ending March 13, about 93% of the 118,000 confirmed cases 12 years and older were in people with two or more doses. But such crude proportions of cases aren’t all that good an indicator of vaccine effectiveness.
Last year, during the Delta outbreak, the proportions were misleading in the other direction. The rate of cases in people who were unvaccinated was about 20 times that in vaccinated people.
Unfortunately, some commentators talked about that ratio as if it was all a real benefit of vaccination. It wasn’t.
The outbreak in Auckland was nearly under control and was spreading among unvaccinated people partly because they had less resistance to infection, but also because they were more likely to come into contact with infected people. Social clustering leads to disease clustering.
What case numbers can tell us
For Delta, two doses of the vaccine produced very good immunity, especially in the short term. The vaccine is less effective for Omicron; two doses give only partial immunity even in the short term, and the effectiveness wears off over time.
About 60% of people 12 years and older have had a booster dose, and in the week ending March 13, only 42% of cases were in people who had been boosted. We can see that boosters help.
Updated vaccine status #covidgraph for week ending 13 March. This very clearly shows the difference boosters make: Unvaxxed are 3.6 x more likely to be in hospital than the boosted. Get your booster people! pic.twitter.com/gOXlVAWzu3
Counting cases remains important, because even a non-hospitalised case of COVID can be unpleasant, and because we don’t know how likely a mild case is to lead to long COVID and months or years of disability. We can’t draw strong conclusions from numbers of cases, though.
Many cases, probably most cases, are not being diagnosed at the moment. Unvaccinated people will be less likely to get tested, especially in mild cases of the disease, either because of poor access to the health system or because they don’t think COVID is important. We can’t really tell how much bias this introduces into the numbers.
Hospitalisations and deaths are much more reliably counted than cases. Results from clinical trials and careful population studies of COVID vaccines consistently show the vaccines to be more effective in preventing more serious disease, especially with the new variants. There are plausible biological explanations for this, based on different parts of our immune response.
Antibodies against the COVID virus seem to be affected more by differences between strains than T-cells are; antibodies are probably more important for preventing initial infection and less important for fighting serious disease.
More benefit in protecting from serious disease
When we look at hospitalisations and deaths, the difference between vaccinated and unvaccinated people is much more dramatic. In the week ending March 13, 65% of people over 12 hospitalised were vaccinated, compared to 94% in the population; 32% had a booster dose, compared to 60% in the population. The 5% of unvaccinated people over 12 contributed 20% of hospitalisations.
The number of deaths is, fortunately, too small for the Ministry of Health to publish detailed weekly breakdowns, but vaccinated people are a minority over the period since August.
The relatively small number of deaths in New Zealand’s Omicron wave also shows the effectiveness of the vaccine. Hong Kong had largely eliminated COVID until Omicron; they are now getting a large outbreak similar to New Zealand’s, but only in the number of cases. Over the past week, Hong Kong averaged 280 deaths per day, in a population less than twice that of New Zealand.
The vaccination rate in Hong Kong is much lower. About 71% are fully vaccinated and only 30% have had a booster. Among elderly people, who are at much greater risk from COVID, the vaccination rate is especially lower, with two-thirds of people over 80 and more than a third of those aged 70-80 having been unvaccinated when Omicron hit.
Towards fair comparisons
Comparing across whole populations this way gives some indication of the vaccine benefit, but it is very imprecise. We don’t choose randomly who gets the vaccine and who doesn’t.
In New Zealand, for example, essentially everyone over 75 has been vaccinated. Since people over 75 are much more likely to need hospital care than younger people, the higher vaccination rate in people over 75 makes the vaccine look less effective than it really is.
Statisticians call this “confounding by indication”. Auckland has always had more exposure to new outbreaks and had higher vaccination rates than the rest of the country; this again tends to make the vaccine look less effective that it really is.
More reliable comparisons require either random allocation of vaccine to people, as in the clinical trials performed before the vaccines were approved, or careful statistical matching of vaccinated and unvaccinated groups to get a fair comparison.
Omicron is too recent to have useful clinical trial data, but peer-reviewed statistical analyses of individual case data from the United Kingdom, the United States, and South Africa all agree the vaccines are beneficial.
There’s some evidence vaccination also reduces the risk and severity of long COVID, the most likely bad outcome for healthy people. But there obviously hasn’t been time to do this sort of comparison specifically for the Omicron variant.
Overall, the most reliable comparisons between vaccinated and unvaccinated people have consistently shown a benefit of vaccination. The effectiveness of the vaccines does wear off over time, and the effectiveness is lower against Omicron than it was against Delta or the original COVID strain, but it still improves your chances of avoiding infection, keeping out of hospital and making a full recovery.
Two more studies, published today in PLOS Medicine show that the reported risks of blood clots following vaccination with anti-COVID vaccination are minuscule and have been greatly exaggerated in the antivaxx disinformation campaigns.
The first study, by William Whiteley of the University of Edinburgh, UK, and colleagues from the BHF Data Science Centre, UK., found, for those under 70, the risk was of the order of 0.9 – 3 per million (varying by age and sex) for AstraZeneca ChAdOx1-S, which is about double the risk for non-vaccinated people. There was no statistically significant increase in the rate of blood clots with Pfizer BNT162b2.
This study analysed the electronic health records of 46 million adults in England of whom 21 million were vaccinated during the study time span, December 2020 to March 2021. For people aged 70 or over, the risks of arterial and venous thrombotic events were slightly lower in the 28 days following vaccination with either the Pfizer BNT162b2 or ChAdOx1-S vaccine.
The second paper, by Steven Kerr of the University of Edinburgh, UK, and colleagues, used a dataset of 11 million adults in England, Scotland, and Wales came to a similar conclusion.
Information provided ahead of publication by PLOS, explains:
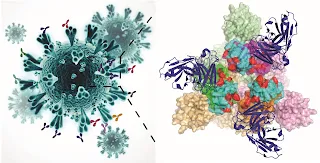
Monoclonal antibody-mediated neutralization of SARS-CoV-2:
The left panel illustrates the morphology of the SARS-CoV-2 virus and displaying the trimeric spike protein on its surface bound with antibodies. The right panel depicts the zoomed view of the trimeric spike protein (top view) in prefusion state bound with monoclonal antibodies. Each monomer of the spike protein shows the receptor binding domain (RBD) in green, orange and magenta, which contains a receptor binding motif in cyan on the top. Mutations emerged in the SARS-CoV-2 Omicron variants are shown in red. Here, the C309 (a parent of VIR-7831 or Sotrovimab) antibody is shown in blue, which is one of the antibodies in clinical use that is minimally impacted by the Omicron variant mutations.
In what may well prove to be a fruitless effort, Anshumali Mittal at the University of Pittsburgh, USA and colleagues have been trying to anticipate how Creationism's beloved pestilential mendacity is likely to modify its SARS-CoV-2 design to make it better at killing people and making others sick, despite the fact that many of them will now have a good degree of immunity, having either been vaccinated against it or acquired it naturally by surviving an earlier attack.
They have been doing so by working out what changes to the spike protein are most likely to enable the virus to evade the antibodies that our immune systems might throw at it in the future
Of course, as any worshiper of the evil genius behind the virus will tell you, it will never give up trying and will always manage to outwit medical science. It's almost exactly like it uses a random process that throws up an almost infinite range of mutations and combinations of mutations, and then something in the environment favours the ones which give most descendants, so even if they are the billion to one chance, the probability that they will arise and become predominant is virtually certain. Rather like repeatedly shuffling the pack and dealing four cards, then repeating until you get four of a kind. It might take days, but if you deal often enough, eventually you will get four of a kind.
Information released ahead of publication in PLOS Pathogens, the PLOS news release explains:
Communities in the North West of England experienced more than three times the excess years of life lost in the South West.
The impact of the COVID-19 pandemic hit hardest in deprived areas of England and Wales, with excess years of life lost more than three times as high in the North West than the South West of England. The research, publishing yesterday in the open access journal PLOS Medicine, also finds 11 times as many excess deaths in 15-44 year olds in the most deprived areas compared to the most affluent ones, and suggests that measuring years of life lost can be more informative for assessing inequalities resulting from the pandemic than looking at excess deaths alone.
According to information made available by PLOS ahead of publication:
Comparing the number of deaths during the pandemic with statistics from previous years can shed light on its impact, but looking at excess deaths alone underestimates years of life lost and does not account for the differences in ages at which people die in different social groups. Evangelos Kontopantelis at the University of Manchester and colleagues looked at mortality registers and estimated expected years of life lost during 2020, by sex, geographical region, and deprivation quintile, using data from Jan 2015 to December 2020.
The impact of the pandemic, when quantified using years of life lost, was higher than previously thought, on the most deprived areas of England and Wales, widening pre-existing health inequalities.
Evangelos Kontopantelis, lead author
Division of Informatics, Imaging and Data Sciences
University of Manchester, Manchester, England, UK
And NIHR School for Primary Care Research
University of Oxford, Oxford, England, UK
The team finds striking socioeconomic and geographical health inequalities, with 1,645 years of life lost per 100,000 of the population in the most deprived areas and 916 years per 100,000 people in the most affluent. London and the North West had the highest years of life lost with South Central and the South West lowest. These inequalities were also seen when examining excess deaths, especially in younger age groups: there were 11 times as many excess deaths in deprived compared to affluent areas in 15-44 year olds, three times as many in 45-64 year olds, almost twice as many in 65-74 year olds, 1.4 times more in 75-84 year olds and no significant difference in people over 85.
Looking at years of life lost is an effective way of determining unmet needs and the authors suggest this could be used for prioritising vaccine delivery and providing targeted financial and social support as part of immediate and longer-term recovery plans. Public health measures and wider socioeconomic interventions are needed to support communities that have been disproportionately affected by the pandemic.
In the abstract to their open access paper, the authors say:
Abstract
Background
Deaths in the first year of the Coronavirus Disease 2019 (COVID-19) pandemic in England and Wales were unevenly distributed socioeconomically and geographically. However, the full scale of inequalities may have been underestimated to date, as most measures of excess mortality do not adequately account for varying age profiles of deaths between social groups. We measured years of life lost (YLL) attributable to the pandemic, directly or indirectly, comparing mortality across geographic and socioeconomic groups.
Methods and findings
We used national mortality registers in England and Wales, from 27 December 2014 until 25 December 2020, covering 3,265,937 deaths. YLLs (main outcome) were calculated using 2019 single year sex-specific life tables for England and Wales. Interrupted time-series analyses, with panel time-series models, were used to estimate expected YLL by sex, geographical region, and deprivation quintile between 7 March 2020 and 25 December 2020 by cause: direct deaths (COVID-19 and other respiratory diseases), cardiovascular disease and diabetes, cancer, and other indirect deaths (all other causes). Excess YLL during the pandemic period were calculated by subtracting observed from expected values. Additional analyses focused on excess deaths for region and deprivation strata, by age-group. Between 7 March 2020 and 25 December 2020, there were an estimated 763,550 (95% CI: 696,826 to 830,273) excess YLL in England and Wales, equivalent to a 15% (95% CI: 14 to 16) increase in YLL compared to the equivalent time period in 2019. There was a strong deprivation gradient in all-cause excess YLL, with rates per 100,000 population ranging from 916 (95% CI: 820 to 1,012) for the least deprived quintile to 1,645 (95% CI: 1,472 to 1,819) for the most deprived. The differences in excess YLL between deprivation quintiles were greatest in younger age groups; for all-cause deaths, a mean of 9.1 years per death (95% CI: 8.2 to 10.0) were lost in the least deprived quintile, compared to 10.8 (95% CI: 10.0 to 11.6) in the most deprived; for COVID-19 and other respiratory deaths, a mean of 8.9 years per death (95% CI: 8.7 to 9.1) were lost in the least deprived quintile, compared to 11.2 (95% CI: 11.0 to 11.5) in the most deprived. For all-cause mortality, estimated deaths in the most deprived compared to the most affluent areas were much higher in younger age groups, but similar for those aged 85 or over. There was marked variability in both all-cause and direct excess YLL by region, with the highest rates in the North West. Limitations include the quasi-experimental nature of the research design and the requirement for accurate and timely recording.
Conclusions
In this study, we observed strong socioeconomic and geographical health inequalities in YLL, during the first calendar year of the COVID-19 pandemic. These were in line with long-standing existing inequalities in England and Wales, with the most deprived areas reporting the largest numbers in potential YLL.
Author summary
Why was this study done?
The Coronavirus Disease 2019 (COVID-19) pandemic generated large numbers of excess deaths (additional deaths over those predicted from trends in previous years). These excess deaths were also unevenly distributed across different geographic areas and socioeconomic groups, exacerbating prepandemic inequalities.
Up to a quarter of the excess deaths during the pandemic were attributable to coronary heart disease, dementia, and other noninfectious causes, and not directly to COVID-19 infection.
Most measures of excess deaths do not fully account for differences in the ages at which people die in different social groups. If the pandemic killed disproportionally more young people in more deprived areas, then inequalities resulting from the pandemic will have been underestimated. Measuring years of life lost (YLL) rather than excess deaths would address this problem.
What did the researchers do and find?
In England and Wales, there were an estimated 763,550 (95% CI: 696,826 to 830,273) excess YLL during the first 42 weeks of the pandemic, of which 15% were not directly attributed to COVID-19 or another respiratory cause.
For all-cause mortality, estimated deaths in the most deprived compared to the most affluent areas were as follows: 11 times as many for 15- to 44-year-olds, 3 times as many for 45- to 64-year-olds, 40% higher in 75- to 84-year-olds, and not significantly higher for those aged 85 or over.
This pattern of disproportionately higher mortality in younger age groups exacerbated prepandemic inequalities between the most and least deprived areas, and varied widely across regions, with the North West particularly affected.
What do these findings mean?
Inequalities between socioeconomic and geographic groups resulting from the COVID-19 pandemic are more pronounced than previously reported.
Future plans to manage pandemics, including decisions about vaccination rollout, should include an understanding of regional and socioeconomic variation in YLL and how this has exacerbated long-standing health inequalities.
Immediate and longer-term recovery planning for communities and their health and social services should reflect historical disparities as well as the impact of the pandemic on YLL.
Limitations of this study include the observational nature of the data and the need for accurate and timely recording of the deaths and their causes.
So, apart from what this says about social inequalities and deprivation in Britain, the message is perfectly clear. Pending the political solution to these inequalities, poor people and young people and especially poor young people should get vaccinated and/or boosted as soon as possible because for them the likely outcome is significantly worse than for people from less deprived backgrounds and the more prosperous areas of the UK.
Her fellow conspiracy theorists have now dreamed up an even more preposterous conspiracy theory: that she is still alive and in 'protective custody' having faked her own death. I wonder if, like Elvis, she'll turn up working in a chip shop near you, in the not too distant future.
Is there no lower limit to the credulity of these idiots? Certainly QAnon hasn't found it yet. They even think Trump was a competent POTUS!
As though any more evidence were needed, two papers out recently show just why it is important to get vaccinated, and, if necessary, boosted against the virus.
The first comes from Washington University School of Medicine in St Louis, Missouri, USA where, by analysing federal health data, researchers have found that people who have had COVID-19 are at increased risk of developing cardiovascular complications within the first month to a year after infection.
According to the Washington University School of Medicine in St Louis:
Scientists at the Massachusetts Institute of Technology (MIT) have discovered how the omicron variant of the SARS-CoV-2 virus, currently causing the largest wave of new and repeat infections yet in the current pandemic, manages to evade the antibodies we produce in response to either vaccinations or earlier infections.
It can do this because of the large number of mutations in the spike proteins that the antibodies would normally bind to, making it difficult for the antibodies to bind to and neutralize the virus particles to prevent them entering the cells.
The article by Anne Trafton of the MIT News Office explains what was discovered and how:
A new study from MIT suggests that the dozens of mutations in the spike protein of the Omicron variant help it to evade all four of the classes of antibodies that can target the SARS-CoV-2 virus that causes Covid-19.
It is important to get a more comprehensive picture of the many mutations seen in Omicron, especially in the context of the spike protein, given that the spike protein is vital for the virus’s function, and all the major vaccines are based on that protein. There is a need for tools or approaches that can rapidly determine the impact of mutations in new virus variants of concern, especially for SARS-CoV-2.
Professor Ram Sasisekharan, Senior author
Alfred H. Caspary professor of Biological Engineering and Health Sciences and Technology
Massachusetts Institute of Technology
Cambridge, MA, USA
This includes antibodies generated by vaccinated or previously infected people, as well as most of the monoclonal antibody treatments that have been developed, says Ram Sasisekharan, the Alfred H. Caspary Professor of Biological Engineering and Health Sciences and Technology (HST) at MIT
Using a computational approach that allowed them to determine how mutated amino acids of the viral spike protein influence nearby amino acids, the researchers were able to get a multidimensional view of how the virus evades antibodies. According to Sasisekharan, the traditional approach of only examining changes in the virus’ genetic sequence reduces the complexity of the spike protein’s three-dimensional surface and doesn’t describe the multidimensional complexity of the protein surfaces that antibodies are attempting to bind to.
[&heelip;]
What’s good about vaccines is they don’t just generate B cells, which produce the monoclonal [antibody] response, but also T cells, which provide additional forms of protection.
With the network approach, you’re looking at that amino acid residue in the context of its neighborhood and environment. When we started to move away from the one-dimensional sequence space toward multidimensional network space, it became evident that critical information about the interaction of an amino acid in its three-dimensional environment in the protein structure is lost when you look at just the one-dimensional sequence space.
Professor Ram Sasisekharan
Even though Omicron is able to evade most antibodies to some degree, vaccines still offer protection, Sasisekharan says.
Antibody escape
After the Omicron variant emerged last November, Sasisekharan and his colleagues began to analyze its trimeric spike protein using a network-based computational modeling method they had originally developed several years ago to study the hemagglutinin spike protein on flu viruses. Their technique allows them to determine how mutations in the genetic sequence are related in the three-dimensional space through a network of inter-amino-acid interactions that critically impact the structure and function of the viral protein.
The researchers’ approach, known as amino acid interaction network analysis, evaluates how one mutated amino acid can influence nearby amino acids depending on how “networked” they are — a measure of how much a given amino acid interacts with its neighbors. This yields richer information than simply examining individual changes in the one-dimensional amino acid sequence space, Sasisekharan says.
[…]
Sasisekharan’s lab has previously used this technique to determine how mutations in the hemagglutinin protein of an avian flu virus could help it to infect people. In that study, he and his laboratory identified mutations that could change the structure of hemagglutinin so that it could bind to receptors in the human respiratory tract.
When Omicron emerged, with about three dozen mutations on the spike protein, the researchers decided to rapidly use their method to study the variant’s ability to evade human antibodies. They focused their analysis on the receptor binding domain (RBD), which is the part of the spike protein targeted by antibodies. The RBD is also the part of the viral protein that attaches to human ACE2 receptors and allows the virus to enter cells.
Using their network modeling approach, the researchers studied how each of the mutations on the RBD changes the protein’s shape and affect its interactions with four classes of human antibodies that target SARS-CoV-2. Class 1 and 2 antibodies target the RBD site that binds to the ACE2 receptor, while class 3 and 4 antibodies bind to other parts of the RBD.
The researchers compared the Omicron variant to the original SARS-CoV-2 virus, as well as the Beta and Delta variants. The Beta and Delta variants have mutations that help them evade class 1 and 2 antibodies, but not class 3 and 4. Omicron, on the other hand, has mutations that affect the binding of all four classes of antibodies.
With Omicron you can see a significant number of sites being perturbed compared to Beta and Delta. From the original strain to the Beta strain, and then the Delta strain, there is a general trend towards a greater ability to escape.
Our hope is that as we understand the viral evolution, we’re able to hone in on regions where we think that any perturbation would cause instability to the virus, so that they would be the Achilles heels, and more effective sites to target.
Professor Ram Sasisekharan
Those perturbations allow the virus to evade not only antibodies generated by vaccination or previous SARS-CoV-2 infection, but also many of the monoclonal antibody treatments that pharmaceutical companies have developed.
As patients began to appear with Omicron infections, researchers and pharmaceutical companies sought to guide treatment by predicting which antibodies were most likely to retain their efficacy against the new variant.
Based on their one-dimensional sequence and single point mutation analyses, pharmaceutical companies believed that their monoclonal antibodies were likely to bind Omicron and not lose any potency. However, when experimental data became available, the Omicron variant was found to substantially escape from monoclonal antibodies known as ADG20, AZD8895, and AZD1061, as predicted by the network analyses in this study, while the activity of monoclonal antibody S309 was also reduced by threefold.
Additionally, the study revealed that some of the mutations in the Omicron variant make it more likely that the RBD will exist in a configuration that makes it easier to grab onto the ACE2 receptor, which may contribute to its enhanced transmissibility.
As any Intelligent [sic] Design advocate will argue, a combination of just the right mutations arising together is so vastly improbable that it must have been intelligently designed. So the Omicron variant must be the intended outcome of intervention by their divine malevolence for the purpose of giving the spiralling arms race between it and medical science, another twist.
Creationist mode:
Of course, as with so many Creationists arguments this ignores reality and relies on ignorant incredulity.
The fact is that, in a process that can produce trillions of new viruses from the few hundreds or thousands in the initial viral load, the one-in-a-billion chance of any particular combination of mutations arising happens a thousand times on average. In a population with millions of unvaccinated people, the probability is very high that a novel variant which is better able to spread and infect people, including those with immunity to the earlier variants, will arise frequently. Omicron is just the latest in a sequence of such variants, and there will be others so long as there is a large pool of unvaccinated people for them to evolve in.
The MIT team's findings are published, open access, in Cell Reports Medicine:
Highlights
Network analyses offer distinct insights into RBD–neutralizing Ab interactions
Omicron mutations broadly and deeply perturb networks across RBD epitope classes
Networks capture indirect effects of Omicron mutations on Ab escape potential
Omicron mutations provide plausible structural rationale for enhanced transmission
Summary
The Omicron variant features enhanced transmissibility and antibody escape. Here, we describe the Omicron receptor binding domain (RBD) mutational landscape using amino acid interaction (AAI) networks, which are well-suited for interrogating constellations of mutations that function in an epistatic manner. Using AAI, we map Omicron mutations directly and indirectly driving increased escape breadth and depth in class 1-4 antibody epitopes. Further, we present epitope networks for authorized therapeutic antibodies and assess perturbations to each antibody’s epitope. Since our initial modeling following the identification of Omicron, these predictions have been realized by experimental findings of Omicron neutralization escape from therapeutic antibodies ADG20, AZD8895, and AZD1061. Importantly, the AAI predicted escape resulting from indirect epitope perturbations was not captured by previous sequence or point mutation analyses. Finally, for several Omicron RBD mutations we find evidence for a plausible role in enhanced transmissibility via disruption of RBD-down conformational stability at the RBDdown-RBDdown interface.
If you are a Creationist, then, you have two choices:
You can ascribe this clearly malevolent piece of redesign to your beloved intelligent [sic] designer and continue to argue that the sheer number of ‘right’ mutations needed to get the desired result proves intelligent intervention. This will tell the world your beloved designer is a malevolent deity who is actively working to make people sick and die and has gone into competition with medical science to make sure it's design keeps on doing that, while ignoring the 'fact' that it also designed the immune system that medical science is using against its design and is now stupidly treating its design, which was intended to protect us against its parasites, as a problem to be overcome.
You can go against the dogmas of your cult and do what people who understand science do - ascribe it to an evolutionary process in which no intelligence or intent was involved - which lets your favourite deity off the hook, explains the appearance of design and explains the uncaring nature of the process and its random victims.
Is fanatical Trumpanzee covidiocy a form of insanity?
I pose this question because Dr Sherri Tenpenny, an osteopath and self-proclaimed expert on the anti-COVID vaccines, who has had no formal training in immunology or epidemiology, puts me in mind of a distressing incident I and my crew mate had to deal with as ambulance Paramedics many years ago. It involved the lawful detention of a female doctor and pathologist under Section 2 of the Mental Health Act (MHA).
The unfortunate lady was being held under Section 136 of the MHA in a local police station as a place of safety, having been apprehended running around the town stark naked and shouting hysterically for people to take cover from an invisible, odourless gas that was pervading the streets and turning them into automatons.
At the peak of the Omicron wave, New York City saw 26 times more deaths among the unvaccinated than vaccinated people. A pop-up COVID-19 testing site is shown in a neighbourhood among those that have seen some of the highest number of city deaths on February 23 in the Queens borough of New York City.
Antivaxx covidiots, scraping around for something to support their selfish stupidity will often point to the fact that vaccinated people are still catching the omicron variant of COVID-19 as evidence that the vaccines don't work. At least only the lunatic fringe conspiracists are still coming up with the more insane claims such as that the vaccine is designed to turn you gay, or make you magnetic so you can be controlled by Bill Gates, or that it is designed to kill you as part of some nefarious eugenic population control.
But what are the merits of this claim of non-effectiveness, as though governments worldwide are spending vast sums of money to give their people something that doesn't work, as well as being in on a vast global conspiracy involving tens or hundreds of millions of people?
The facts are, as explained in this Newsweek report, not on the side of the antivaxxers, not because they are wrong to claim that vaccinated people can still catch COVID-19, but because they are wrong to claim this means the vaccines are not effective.
In fact, the evidence is that, as the vaccine manufacturers always claimed, that, while not 100% effective and while not giving permanent protection as immunity was likely to decline over time, so top-up boosters will be needed, the vaccines give you a very significantly increased probability of avoiding serious illness and death. And this is borne out by the facts, both in the USA and in the UK.
My first two anti-COVID vaccines were the Astra-Zeneca vaccines but, for reasons of availability, my booster was the Pfizer vaccine. None of the vaccines caused anything more than the slightest discomfort at the injection site which lasted about 2 days. However, a friend of mine declined an offered booster because it wasn’t the same as the initial vaccine and thought there might be a smaller boost as well as doubling the risk of an adverse reaction.
So, which of us was right?
The preliminary results of a clinical trial by the US National Institute of Health, show that there is certainly no disadvantage in a mix and match approach and there may even be a benefit. The trial results are reported in The New England Journal of Medicine.
A second research group has reported that vaccinations against COVID-19 given before or after breakthrough infections, significantly enhances antibody levels, again making the case for vaccination unarguable. Readers may remember how I reported on a similar paper a few days ago.
This time the research comes from the Oregon Health & Science University (OHSU), Portland, Oregon, USA. The team found that it makes little difference whether you have the vaccine after being infected with SARS-CoV-2 or whether you are unlucky enough to get a 'breakthrough' infection after having been vaccinated. However, with the virus now being so common in the environment, the chance of a breakthrough infection, post vaccine is high, though not as high as for an unvaccinated person. Without the vaccine, however, natural immunity following infection is much lower.
It makes no difference whether you get infected and then vaccinated, or if you get vaccinated and then a breakthrough infection. In either case, you will get a really, really robust immune response — amazingly high.
The likelihood of getting breakthrough infections is high because there is so much virus around us right now, but we position ourselves better by getting vaccinated. And if the virus comes, we’ll get a milder case and end up with this super immunity.
Fikadu Tafesse, Ph.D., Senior author
Assistant professor of molecular microbiology and immunology
OHSU School of Medicine
Portland, Oregon, USA
The OHSU news release accompanying the team's open access publication, in the journal Science Immunology, explains:
It's beginning to look like Creationism's divine malevolence may have blundered badly in its eagerness to modify the SARS-CoV-2 virus so it could overcome the vaccines made by medical science and kill more people and leave more with long-term disabilities.
At least this has to be the conclusion for Creationists who are obliged by dogma to reject the idea that a natural, evolutionary process could be behind the modifications which can only occur if their putative intelligent (sic) supernatural designer makes the changes.
Our study provides for the first time an explanation, why Omicron infections are less likely to cause severe disease. Obviously, Omicron can in contrast to Delta not effectively inhibit the host cell interferon immune response.
Prof Martin Michaelis, co-Lead author
School of Bioscience
University of Kent
Canterbury, Kent, UK
Scientists from the University of Kent and the Goethe University, Frankfurt have shown that the SARS-CoV-2 omicron variant is less effective than delta at blocking a cellular defence mechanism against viruses - the so-called “interferon response”.
The researchers have shown that omicron variant viruses are particularly sensitive to inhibition by the so-called interferon response, an unspecific immune response that is present in all body cells. This provides the first explanation of why COVID-19 patients infected with the omicron variant are less likely to experience severe disease.
A couple of weeks ago, Cirsten Weldon, a vociferous Pro-Trump QAnon conspiracist and antivaxxer, died in hospital of COVID-19, another in a long line of similar covidiot antivaxx nutters, so doing their bit for the self-inflicted genocide being waged by Trumpanzee cult loons against their own core supporters.
Scientists working at the University of Washington Medical School (UW Medicine), Washington, USA, have shown that either a third (booster) vaccination or infection with SARS-CoV-2 gives comparable magnitude and breadth of protection, but those who have been vaccinated twice but still get a breakthrough infection usually do not have a severe infection.
Of course, anyone who is unfortunate enough to get a breakthrough infection or who is unvaccinated, runs a far higher risk of serious illness and long-term complications than those who have all three vaccinations, so the case for vaccination remains unarguable. The news release from UW Medicine explains: