May 17 2020 Donald Trump praised protesters who harassed a journalist on Long Island this week at a rally where one man called for the execution of Dr. Anthony Fauci.
One of the more enduring and insidious legacies of the disastrous single-term US president, Donald J. Trump, is that distrusting public Health Officials who tried to explain the science behind the COVID-19 pandemic and the measures to mitigate it, and by extension, all scientists, to the extent of harassing them, attacking them, and even making death threats against them when they deliver unwelcome news, has now become acceptable to a significant proportion of American adults.
That proportion appears to be growing according to an investigation by scientists from Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, USA, the University of Colorado, Aurora, Colorado, USA, the Weill Cornell Medical College, New York, New York, USA and the Cornell Jeb E. Brooks School of Public Policy, Ithaca, New York, USA. Their findings are published open access in the online Journal of the American Medical Association (JAMA) Open Network.
Their key findings were:
Key Points
Question What factors shape US adults’ beliefs regarding whether threatening or harassing public health officials was justified during the COVID-19 pandemic?
Findings In this survey study of 1086 US adults, the share who believed that harassing or threatening public health officials because of business closures was justified rose from 20% to 25% and 15% to 21%, respectively, from November 2020 to July and August 2021. There were increases in negative views over time among higher earners, political independents, those with more education, and those most trusting of science.
Meaning These findings suggest that restoring trust in public health officials will require strategies tailored to engage diverse viewpoints.
They give more detail in the abstract to their paper:
Figures provided a few days ago by investigators from the University of California San Diego, show that health care facilities serving underrepresented, rural and hardest-hit communities in the USA were less likely to administer COVID-19 vaccines in the early phase of the vaccine rollout and that the reason could well have been the lower availability of sites having vaccines to administer, rather than vaccine hesitancy or distrust, as has previously been suggested.
In particular, there were significantly fewer vaccination facilities in rural counties that were predominantly black or Hispanic and even where the mortality figures for COVID-19 were highest.
As the UC San Diego press release explains:
Proportion of facilities serving as COVID-19 vaccine administration locations.
When reports showed COVID-19 vaccination rates were lower among racial/ethnic minority groups, most discussions focused on mistrust and misinformation among these populations or their reduced access to health care facilities. But new research from University of California San Diego and collaborating institutions has identified an additional barrier to equity: whether or not each health care facility actually received and administered vaccines.
[…]
In a study published July 28, 2022 in PLOS Medicine, researchers demonstrated that health care facilities serving underrepresented, rural and hardest-hit communities were less likely to administer COVID-19 vaccines in the early phase of the vaccine rollout.
Led by Inmaculada Hernandez, PharmD, PhD, associate professor of clinical pharmacy at Skaggs School of Pharmacy and Pharmaceutical Sciences at University of California San Diego, the study is the first to quantify disparities in the early distribution of COVID-19 vaccines to health care facilities across the country.
Previous studies of vaccine accessibility have not distinguished whether lower access in underserved neighborhoods was a product of the lower concentration of health care facilities in these areas or of inequities in the distribution of COVID-19 vaccines to each health care facility.
To answer this question, Hernandez and colleagues tested whether the likelihood of an eligible health care facility administering COVID-19 vaccines varied based on the racial/ethnic composition and urbanicity of the local county. The team focused on the initial phase of vaccine rollout, using data from May 2021 when states were officially required to make vaccines available to the public.
At that time, 61 percent of eligible health care facilities and 76 percent of eligible pharmacies across the U.S. provided COVID-19 vaccinations. When researchers began comparing these rates with the socioeconomic features of the county each facility was located in, several patterns emerged.
Both the national policy and public opinion agreed that vaccine distribution should prioritize disadvantaged communities and those hit hardest by COVID-19, but the data shows that is not what happened.
Dr Inmaculada Hernandez, PharmD, PhD, lead author
Associate professor of clinical pharmacy
Skaggs School of Pharmacy and Pharmaceutical Sciences
University of California San Diego, San Diego, CA, USA
Facilities in counties with a high proportion of Black people were less likely to serve as COVID-19 vaccine administration locations compared to facilities in counties with a low proportion of Black people. This was particularly the case in metropolitan areas, where facilities in urban counties with large Black populations had 32 percent lower odds of administering vaccines compared to facilities in urban counties with small Black populations.
To achieve health equity in future public health programs, including the distribution of booster shots, it is crucial that public health authorities review these early COVID-19 distribution plans to understand how and why this happened.
Dr Jingchuan (Serena) Guo, MD, PhD, senior author
Assistant professor
University of Florida, FL, USA
Facilities in rural counties and in counties hardest hit by COVID-19 were also associated with decreased odds of serving as a COVID-19 vaccine administration location. In rural counties with a high proportion of Hispanic people, facilities had 26 percent lower odds of administering vaccines compared to facilities in rural counties with a low proportion of Hispanic people.
Further research is necessary to identify the reasons why vaccines were not equitably distributed to all health care facilities and how the involvement of these facilities evolved across subsequent phases of vaccine distribution, the authors said.
The following charts show the researchers' findings (click the buttons for greater clarity):
Fig 1. Adjusted odds ratios of facilities serving as COVID-19 vaccine administration locations, main effects.
The figure shows the results of logistic regression models fitted with generalized estimating equations for the primary outcome of a healthcare facility (or a pharmacy) serving as a COVID-19 vaccine administration location. The model only included main effects. All healthcare facilities included pharmacies, FQHCs, RHCs, and HODs. The circles represent the point estimate for the odds ratio, and the whiskers represent the 95% confidence interval. COVID-19, Coronavirus Disease 2019; FQHC, federally qualified health center; HOD, hospital outpatient department; RHC, rural health clinic.
Fig 2. Adjusted odds ratios of facilities serving as COVID-19 vaccine administration locations, interaction for proportion non-Hispanic Black population and urbanicity.
The figure shows the results of logistic regression models fitted with generalized estimating equations for the primary outcome of a healthcare facility (or a pharmacy) serving as a COVID-19 vaccine administration location. All healthcare facilities included pharmacies, FQHCs, RHCs, and HODs. The model adjusted for all covariates listed in Fig 1. Additionally, the model constructed for all healthcare facilities included an indicator variable for facility type (pharmacy vs. others). The circles represent the point estimate for the odds ratio, and the whiskers represent the 95% confidence interval. COVID-19, Coronavirus Disease 2019; FQHC, federally qualified health center; HOD, hospital outpatient department; RHC, rural health clinic.
Fig 3. Adjusted odds ratios of facilities serving as COVID-19 vaccine administration locations, interaction for proportion Hispanic population and urbanicity.
The figure shows the results of logistic regression models fitted with generalized estimating equations for the primary outcome of a healthcare facility (or a pharmacy) serving as a COVID-19 vaccine administration location. All healthcare facilities included pharmacies, FQHCs, RHCs, and HODs. The model adjusted for all covariates listed in Fig 1. Additionally, the model constructed for all healthcare facilities included an indicator variable for facility type (pharmacy vs. others). The circles represent the point estimate for the odds ratio, and the whiskers represent the 95% confidence interval. COVID-19, Coronavirus Disease 2019; FQHC, federally qualified health center; HOD, hospital outpatient department; RHC, rural health clinic.
More detail is given in the abstract and authors' summary in the team's open access paper in PLOS Medicine:
Abstract
Background
The US Centers for Disease Control and Prevention has repeatedly called for Coronavirus Disease 2019 (COVID-19) vaccine equity. The objective our study was to measure equity in the early distribution of COVID-19 vaccines to healthcare facilities across the US. Specifically, we tested whether the likelihood of a healthcare facility administering COVID-19 vaccines in May 2021 differed by county-level racial composition and degree of urbanicity.
Methods and findings
The outcome was whether an eligible vaccination facility actually administered COVID-19 vaccines as of May 2021, and was defined by spatially matching locations of eligible and actual COVID-19 vaccine administration locations. The outcome was regressed against county-level measures for racial/ethnic composition, urbanicity, income, social vulnerability index, COVID-19 mortality, 2020 election results, and availability of nontraditional vaccination locations using generalized estimating equations.
Across the US, 61.4% of eligible healthcare facilities and 76.0% of eligible pharmacies provided COVID-19 vaccinations as of May 2021. Facilities in counties with >42.2% non-Hispanic Black population (i.e., > 95th county percentile of Black race composition) were less likely to serve as COVID-19 vaccine administration locations compared to facilities in counties with >12.5% non-Hispanic Black population (i.e., lower than US average), with OR 0.83; 95% CI, 0.70 to 0.98, p = 0.030. Location of a facility in a rural county (OR 0.82; 95% CI, 0.75 to 0.90, p < 0.001, versus metropolitan county) or in a county in the top quintile of COVID-19 mortality (OR 0.83; 95% CI, 0.75 to 0.93, p = 0.001, versus bottom 4 quintiles) was associated with decreased odds of serving as a COVID-19 vaccine administration location.
There was a significant interaction of urbanicity and racial/ethnic composition: In metropolitan counties, facilities in counties with >42.2% non-Hispanic Black population (i.e., >95th county percentile of Black race composition) had 32% (95% CI 14% to 47%, p = 0.001) lower odds of serving as COVID administration facility compared to facilities in counties with below US average Black population. This association between Black composition and odds of a facility serving as vaccine administration facility was not observed in rural or suburban counties. In rural counties, facilities in counties with above US average Hispanic population had 26% (95% CI 11% to 38%, p = 0.002) lower odds of serving as vaccine administration facility compared to facilities in counties with below US average Hispanic population. This association between Hispanic ethnicity and odds of a facility serving as vaccine administration facility was not observed in metropolitan or suburban counties.
Our analyses did not include nontraditional vaccination sites and are based on data as of May 2021, thus they represent the early distribution of COVID-19 vaccines. Our results based on this cross-sectional analysis may not be generalizable to later phases of the COVID-19 vaccine distribution process.
Conclusions
Healthcare facilities in counties with higher Black composition, in rural areas, and in hardest-hit communities were less likely to serve as COVID-19 vaccine administration locations in May 2021. The lower uptake of COVID-19 vaccinations among minority populations and rural areas has been attributed to vaccine hesitancy; however, decreased access to vaccination sites may be an additional overlooked barrier.
Author summary
Why was this study done?
Equity in the distribution of Coronavirus Disease 2019 (COVID-19) vaccine is of major relevance.
It is unknown whether there were differences in the distribution of COVID-19 vaccines to healthcare facilities depending on the demographic composition of the population.
What did the researchers do and find?
We tested whether healthcare facilities serving minority or disadvantaged neighborhoods were less likely to administer COVID-19 vaccines in the early phase of the COVID-19 vaccine rollout process.
We found that healthcare facilities in counties with higher Black composition, in rural areas, and in hardest-hit communities were less likely to administer COVID-19 vaccines in May 2021.
What do these findings mean?
There were disparities in the early distribution of COVID-19 vaccines to healthcare facilities across the country.
From these figures it is clear that there was a differential in the availability of vaccines between the wealthier, white and less deprived areas of the USA and the predominantly black, deprived areas and that even differences in mortality rates did not reverse that trend. It is also clear that there was a differential based on voting patterns in the 2020 presidential elections.
More research is now needed to determine whether this was due to political/racial prejudice on behalf of the suppliers or on behalf of the local authorities responsible for requesting supplies of the vaccine and providing facilities for their administration, and to what extent Donald Trump's disastrous lead in downplaying the seriousness of the pandemic to cover for his own incompetence, played a part in this disparity.
But, whatever the cause, it is clear that, in the early phase of the vaccine roll-out, there was not equitable distribution of the vaccines and that racial minorities and people in deprived areas of the USA and in Trump-supporting counties were least likely to get them.
While to most children, COVID-19 is a relatively mild illness, a significant number become ill enough to be admitted to hospital. According to an international study led by Dr Anna Funk, PhD, an epidemiologist and University of Calgary postdoctoral fellow, of those who were hospitalised for 48 hours or more, had 4 or more symptoms at the initial Emergency Department (ED) assessment and were aged 14 years or older, 60% went on to develop 'Long Covid' and show symptoms 90 days later.
The results of the study were published yesterday in the open access Journal of the American Medical Association (JAMA Network Open).
According to UCalgary News:
We found that in some children, illness with COVID-19 is associated with reporting persistent symptoms after three months.
Our results suggest that appropriate guidance and followup are needed, especially for children at high risk for long COVID.
Dr. Stephen Freedman, MD, principal investigator
Paediatric emergency medicine physician
Alberta Health Services
And associate professor of medicine
Cumming School of Medicine (CSM).
The study included 1,884 children with COVID-19 who had 90-day followup. Long COVID was found in nearly 10 per cent of hospitalized children and five per cent in children discharged from the ED.
Reported rates of long COVID in adults are substantially higher than what we found in children.
Our findings can inform public health policy decision regarding COVID-19 mitigation strategies for children and screening approaches for long COVID among those with severe outcomes.
Dr. Nathan Kuppermann, MD, MPH, co-principal investigator
University of California
Davis School of Medicine, Sacramento.
Our finding that children who had multiple COVID-19 symptoms initially were at higher risk for long COVID is consistent with studies in adults.
Unfortunately, there are no known therapies for long COVID in children and more research is needed in this area. However, if symptoms are significant, treatment targeting the symptoms is most important. Multidisciplinary care is warranted if symptoms are impacting quality of life.
Dr. Todd Florin, MD, MSCE, co-principal investigator
Ann & Robert H. Lurie Children’s Hospital
Chicago and Northwestern University Feinberg School of Medicine.
The most-reported persistent symptoms in children were fatigue or weakness, cough, difficulty breathing or shortness of breath.
More technical detail is given in the study report in JAMA Network Open:
Key Points
Question What proportion of children infected with SARS-CoV-2 who were tested in emergency departments (EDs) reported post–COVID-19 conditions (PCCs) 90 days after their ED visits?
Findings In this cohort study of 1884 SARS-CoV-2–positive children with 90-day follow-up, 5.8% of patients, including 9.8% of hospitalized children and 4.6% of discharged children, reported PCCs. Characteristics associated with PCCs included being hospitalized 48 hours or more, having 4 or more symptoms reported at the index ED visit, and being 14 years of age or older.
Meaning This study suggests that, given the prevalence of PCCs, appropriate guidance and follow-up are required for children testing positive for SARS-CoV-2.
Abstract
Importance Little is known about the risk factors for, and the risk of, developing post–COVID-19 conditions (PCCs) among children.
Objectives To estimate the proportion of SARS-CoV-2–positive children with PCCs 90 days after a positive test result, to compare this proportion with SARS-CoV-2–negative children, and to assess factors associated with PCCs.
Design, Setting, and Participants This prospective cohort study, conducted in 36 emergency departments (EDs) in 8 countries between March 7, 2020, and January 20, 2021, included 1884 SARS-CoV-2–positive children who completed 90-day follow-up; 1686 of these children were frequency matched by hospitalization status, country, and recruitment date with 1701 SARS-CoV-2–negative controls.
Exposure SARS-CoV-2 detected via nucleic acid testing.
Main Outcomes and Measures Post–COVID-19 conditions, defined as any persistent, new, or recurrent health problems reported in the 90-day follow-up survey.
Results Of 8642 enrolled children, 2368 (27.4%) were SARS-CoV-2 positive, among whom 2365 (99.9%) had index ED visit disposition data available; among the 1884 children (79.7%) who completed follow-up, the median age was 3 years (IQR, 0-10 years) and 994 (52.8%) were boys. A total of 110 SARS-CoV-2–positive children (5.8%; 95% CI, 4.8%-7.0%) reported PCCs, including 44 of 447 children (9.8%; 95% CI, 7.4%-13.0%) hospitalized during the acute illness and 66 of 1437 children (4.6%; 95% CI, 3.6%-5.8%) not hospitalized during the acute illness (difference, 5.3%; 95% CI, 2.5%-8.5%). Among SARS-CoV-2–positive children, the most common symptom was fatigue or weakness (21 [1.1%]). Characteristics associated with reporting at least 1 PCC at 90 days included being hospitalized 48 hours or more compared with no hospitalization (adjusted odds ratio [aOR], 2.67 [95% CI, 1.63-4.38]); having 4 or more symptoms reported at the index ED visit compared with 1 to 3 symptoms (4-6 symptoms: aOR, 2.35 [95% CI, 1.28-4.31]; ≥7 symptoms: aOR, 4.59 [95% CI, 2.50-8.44]); and being 14 years of age or older compared with younger than 1 year (aOR, 2.67 [95% CI, 1.43-4.99]). SARS-CoV-2–positive children were more likely to report PCCs at 90 days compared with those who tested negative, both among those who were not hospitalized (55 of 1295 [4.2%; 95% CI, 3.2%-5.5%] vs 35 of 1321 [2.7%; 95% CI, 1.9%-3.7%]; difference, 1.6% [95% CI, 0.2%-3.0%]) and those who were hospitalized (40 of 391 [10.2%; 95% CI, 7.4%-13.7%] vs 19 of 380 [5.0%; 95% CI, 3.0%-7.7%]; difference, 5.2% [95% CI, 1.5%-9.1%]). In addition, SARS-CoV-2 positivity was associated with reporting PCCs 90 days after the index ED visit (aOR, 1.63 [95% CI, 1.14-2.35]), specifically systemic health problems (eg, fatigue, weakness, fever; aOR, 2.44 [95% CI, 1.19-5.00]).
Conclusions and Relevance In this cohort study, SARS-CoV-2 infection was associated with reporting PCCs at 90 days in children. Guidance and follow-up are particularly necessary for hospitalized children who have numerous acute symptoms and are older.
Funk AL, Kuppermann N, Florin TA, et al.
Post–COVID-19 Conditions Among Children 90 Days After SARS-CoV-2 Infection. JAMA Netw Open. 2022; 5(7): e2223253. doi: 10.1001/jamanetworkopen.2022.23253
The irony is it is more or less the same antivaxxer covidiots who were jubilant when SCOTUS effectively took away the right of American women to plan their parenthood on the grounds that they were 'pro-life', who are campaigning to persuade people to risk their children's lives and welfare by not getting vaccinated against COVID-19. Clearly, these people don't really believe in the sanctity of life; what they believe in is imposing their will on other people. Religion merely provides them with the excuse they need.
Although the figures above are statistically interesting, I would suggest the only one that should interest responsible, loving parents is the one that shows your children run a significant risk of contracting 'Long COVID' if they become infected. Other studies have shown that all the vaccines are effective at reducing the risk of a serious breakthrough infection, so there really is no valid argument:
Don't be a Covidiot! Get vaccinated and get your children vaccinated, now!
Be under no illusions, the COVID-19 pandemic is far from over.
We are currently seeing yet another wave of infections as the Omicron variant diverges into new and even more infections variants, and investigators at the US National Insitute of Allergy and Infectious Diseases have shown that the antibody levels following vaccination wane significantly in about 3 months.
Under the influence of his scientific illiteracy and political incompetence during the COVID-19 pandemic, former President Donald Trump's lasting legacy is likely to be a large and growing number of Americans who now distrust science and so represent a danger to the rest of us.
The result is a growing resistance to measures to combat climate change and vaccination campaigns to eradicate or control pandemic such as the current coronavirus pandemic or life-threatening epidemics such as measles, mumps and rubella.
This level of anti-science attitude in a major country is a clear danger to the world as a whole, since climate change and viruses are not limited by national borders.
Now three researchers at Ohio State University who study attitudes and persuasion, have published a paper in Proceeding of the National Academy of Science (PNAS) which explain the rise in anti-science beliefs today and outlines what can be done about it. Sadly, the paper itself is behind an expensive paywall, but the abstract is available, open access, under a Creative Commons licence.
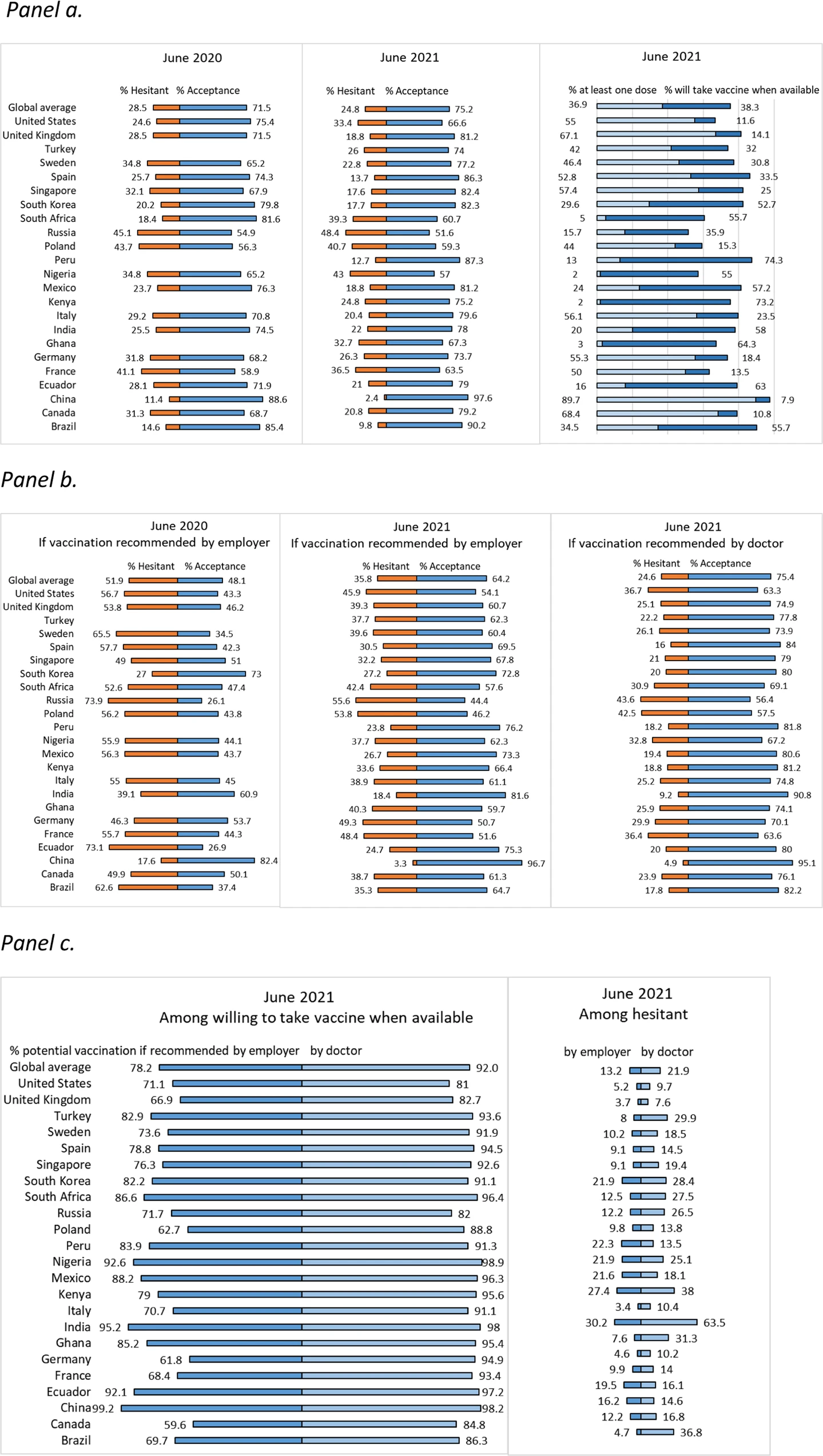
a COVID-19 vaccine hesitancy and acceptance. b COVID-19 vaccine hesitancy and acceptance if recommended by employer or one’s doctor. a, b COVID-19 acceptance in June 2020 was defined as willingness to take vaccine if proven safe and effective. COVID-19 vaccine acceptance in June 2021 was defined as having received at least one dose of a COVID-19 vaccine and if not, willingness to take the COVID-19 vaccine when it is available to them. Vaccine hesitancy was defined as having reported “no” to the question on whether they have received at least one dose of a COVID-19 vaccine and also either unsure/no opinion, somewhat disagree, or strongly disagree to the question on whether they would take a COVID-19 vaccine when available to them. Four countries (Ghana, Kenya, Peru, and Turkey) were not included in the 2020 global survey. c Potential COVID-19 vaccine acceptance if recommended by employer or one’s doctor among those willing to take vaccine when available and those hesitant to vaccinate. c Potential COVID-19 vaccination was defined as willingness to take the COVID-19 vaccine when it is available if recommended by employer or by doctor.
A new study by scientists from the City University of New York School of Public Health (CUNY SPH), USA, the Barcelona Institute for Global Health (ISGlobal), Hospital Clínic, University of Barcelona, Barcelona, Spain, the University of Calgary, Calgary, Alberta, Canada and the School of Health Administration, Dalhousie University, Halifax, Nova Scotia, Canada, has show a growing acceptance of the anti-Covid vaccines on a global scale between 2020 and 2021.
The team conducted a survey of 23,000 individuals from 23 countries in June 2021 and found that 75.2% reported acceptance of the vaccine, compared to 71.5% in 2020. The results of the survey were published open access in Nature Communications.
According to the CUNY SPH press release:
The study … was carried out within the context of a year of substantial but very unequal global COVID-19 vaccine availability and acceptance, which necessitated new assessments of the drivers of vaccine hesitancy and the characteristics of people not vaccinated.
Concerns about vaccine safety and efficacy and mistrust in the science behind vaccine development were the most consistent correlates of hesitancy. Other factors associated with vaccine hesitancy varied by country and included personal experience with COVID-19 (e.g., sickness or loss of a family member) and demographic characteristics (e.g., gender, education, and income).
The authors found that vaccine hesitancy did not significantly correlate with a country’s current COVID-19 case burden and mortality. In June 2021, vaccine hesitancy was reported most frequently in Russia (48.4%), Nigeria (43%), and Poland (40.7%), and least often in China (2.4%), the United Kingdom (UK) (18.8%), and Canada (20.8%).
In order to improve global vaccination rates, some countries may at present require people to present proof of vaccination to attend work, school, or indoor activities and events. Our results found strong support among participants for requirements targeting international travellers, while support was weakest among participants for requirements for schoolchildren.
Jeffrey Lazarus, lead author.
Barcelona Institute for Global Health (ISGlobal)
Hospital Clínic
University of Barcelona, Barcelona, Spain
And the Graduate School of Public Health & Health Policy
City University of New York (CUNY), New York, NY, US
Support for vaccine mandates was substantially lower among those who were hesitant to get vaccinated themselves.
Importantly, however, recommendations by a doctor, or to a lesser extent by an employer, might have an impact on a respondent’s views on vaccination in some countries.
Dean Ayman El-Mohandes, co-author
Graduate School of Public Health ∓ Health Policy
City University of New York (CUNY), New York, NY, USA
Although some countries are currently disengaging from evidence-based COVID-19 control measures, the disease has by no means been controlled or ended as a public health threat. The authors note that for ongoing COVID-19 vaccination campaigns to succeed in improving coverage going forward, substantial challenges remain. These include targeting those reporting lower vaccine confidence with evidence-based information campaigns and greatly expanding vaccine access in low- and middle-income countries.
Covid-19 vaccination during pregnancy reduced the risk of hospitalisation with COVID-19 for babies under 6 month-old by 80% for the Delta variant and by 40% for the Omicron variant.
Contrary to the antivaxx propaganda coming from the extreme right in the USA, a new study, sponsored by the US Center for Disease Control and Prevention (CDC), has shown that COVID-19 vaccination during pregnancy reduced the risk of babies under 6 month old needing hospitalization due to COVID-19 infection, by 80% during the Delta wave and 40% during the Omicron wave.
The study, led by Dr. Bria M. Coates, MD, was conducted by investigators from the Ann & Robert H. Lurie Children’s Hospital, Chicago and the Northwestern University Feinberg School of Medicine, Chicago. It included infants younger than 6 months of age who were admitted to 30 paediatric hospitals in 22 states from July 1, 2021, to March 8, 2022. Dr Coates and his colleagues found that most infants (90 percent) who needed intensive care due to COVID-19 infection were born to mothers who were not vaccinated during pregnancy.
Figures published yesterday in eLife, show that, during the Delta variant wave of COVID-19 in the summer of 2021, areas with a high level of vaccine take-up in the USA had a lower peak of hospitalisations and deaths, and a shorter duration of the wave, compared to areas where the take-up was low.
The summer of 2021 was of course when pro-Trump QAnon, antivaxxers and evangelical Christians were loudest in campaigning to mislead people about the severity of the pandemic and the effectiveness/harmful effects of the COVID-19 vaccine, as a direct consequence of then president Trump's incompetent response to the crisis where he was out of his depth, so sought to minimise it to justify his inaction and indecision, so setting the scene for his supporters in the far right Trumpanzee cults. Consequently, those parts of America where a large number of people, mostly Trumpanzee Republicans, were refusing to get vaccinated or take sensible precautions against catching the virus and passing it on to others.
Now figures are showing the harm that did to those who fell for the lies emanating from the White House, and so made themselves vulnerable to the potentially life-threatening condition.
A new study from UCLA researchers indicates a previously undocumented impact of widespread Covid-19 vaccine promotion on other public health behaviours. Adult flu vaccination rates have declined in states with low rates of Covid-19 vaccination, which the authors say may be a harbinger of declining trust in public health, suggesting that Covid-19 vaccination behaviour has spilled over to flu vaccination behaviour. The finding is published in The New England Journal of Medicine as a letter to the editor.
States with a low COVID-19 take-up are, of course, mostly red states where a majority of voters think Trump was a good president, so have been easy victims for the right-wing frauds who spread antivaxx disinformation and claim the pandemic was a conspiracy and the measure to combat it were unnecessary and an attack on their freedoms. These are also the fools who believed the right-wing political rhetoric of the pro-Trump evangelical white Christian churches who said it was all a plot to close the churches and to prevent Christians from practicing their faith.
It is alarming that controversy surrounding Covid-19 vaccination may be undermining separate public health efforts that save thousands of lives each year. Many Americans who never before declined a routine, potentially life-saving vaccine have started to do so. This supports what I have seen in my clinical practice and suggests that information and policies specific to Covid-19 vaccines may be eroding more general faith in medicine and our government’s role in public health.
Much as someone’s decision to wear or forgo a mask in public during the early pandemic was linked with their more general beliefs through the idea of ‘belief signaling’, we propose that ‘belief generalization’ may account for Covid-19 vaccine-specific opinions being generalized to other vaccines. People who feel compelled to oppose or support Covid-19 vaccines may feel that they should in turn oppose or support other vaccines.
Dr Richard Leuchter, MD, lead author
A resident physician at UCLA Health
And the David Geffen School of Medicine.
The letter to the editor of The New England Journal of Medicine points out how these fools have been victimised twice - one over the COVID-19 vaccine and again over the trustworthiness of medical science and in particular the flu vaccines which have done so much to prevent a serious flu pandemic by giving annual flu jabs to combat the latest, or most likely new flu variants.
According to the UCLA Health press release:
The authors used publicly available data from the Centers for Disease Control and Prevention (CDC) collected through January 2022 to evaluate how flu vaccination rates changed during the pandemic based on state-wide rates of Covid-19 vaccination.
Flu vaccination rates for the first flu season of the pandemic (2020-2021), which pre-dated the widespread availability of Covid-19 vaccines, remained relatively stable across all states. However, in the second flu season of the pandemic (2021-2022), which was after widespread promotion of Covid-19 vaccines, flu vaccination rates dropped 4.5 percentage points (from 43.7% to 39.2%) in states with below-average rates of Covid-19 vaccination. Conversely, states with the highest uptake of Covid-19 vaccines saw increases in average flu vaccination rates of 3.8 percentage points (from 49.0% to 52.8%).
The authors say these findings taken together suggest that Covid-19 vaccination behaviors have spilled over to other public health behaviors, in this case flu vaccination. They explain that this relationship works in both directions: factors causing low Covid-19 vaccination rates (e.g., mistrust of Covid-19 vaccines, concerns about side effects, lack of trust in government) are linked to declines in flu vaccination compared to pre-pandemic times, whereas factors causing high rates of Covid-19 vaccination are spilling over to increase flu vaccination rates.
The authors propose that both of these trends may be explained by something called belief generalization.
It takes a special kind of stupid to think that, even if COVID-19 vaccinations are unnecessary and/or don't work or are part of some nefarious Satanic plot (which admittedly takes a high level of credulous gullibility in the first place) that this means flu jabs should be avoided too. But then we are still talking about people who think Trump was a good president, so for whom evidence is of no consequence and what they're taught to think from the pulpit is definitive truth.
The press release continues:
This is compelling evidence that the vaccination behaviors for flu and Covid-19 vaccines are inextricably linked.
Dr Richard Leuchter, MD
Rates of full vaccination against Covid-19 (i.e., both doses of a two-dose vaccine or one dose of a single-dose vaccine) varied from 50% (Alabama) to 81% (Rhode Island) through January 2022. Flu vaccination rates through January of the 2021-2022 flu season were also highly variable, ranging from 31% (Mississippi) to 59% (Connecticut). The study authors found that 60% of the variation in a state’s flu vaccination rate could be explained solely by that state’s average Covid-19 vaccination rate.
The authors note that these findings apply only to the general adult population. Flu vaccination rates among children fell uniformly and precipitously across both the 2020-2021 and 2021-2022 flu seasons, regardless of when Covid-19 vaccines were introduced or state-wide rates of Covid-19 vaccination. The authors point out that previous studies have reported similar dramatic national declines in rates of childhood vaccination against measles, mumps, and rubella (MMR). Leuchter says that while belief generalization in the negative direction may partially explain why parents are opting out of routine vaccines for their children, the fact that childhood flu vaccination declined even among states with high rates of Covid-19 vaccination suggests that belief generalization from Covid-19 vaccines does not fully account for this trend. Reassuringly, flu vaccination rates among adults over 65 years of age remained relatively stable during these two flu seasons compared to the 2019-2020 season, albeit persistently underutilized in this population.
This study had some limitations. For instance, it did not directly measure individuals’ beliefs or reasons for forgoing vaccination. As an observational study, it does not prove that lack of trust of the vaccines or government caused the new decline in flu vaccination rates. In addition, the CDC reports flu vaccination rates based on self-report surveys and has not made county-level data for the 2021-2022 flu season available, so only state-wide data were used.
Despite these limitations, the researchers state that these findings should raise alarm and prompt rigorous study of the causes of decreases in non-Covid-19 vaccination rates to inform urgent action and corrective policies.
Sadly the letter in The New England Journal of Medicine is protected by copyright so can't be reproduced here. However, in their open paragraph, the authors make it clear that they place responsibility for this situation on the polarization of opinion over COVID-19:
The polarizing nature of vaccination against coronavirus disease 2019 (Covid-19) within the United States threatens public health and has contributed to variable statewide vaccine uptake that ranged from 50 to 80% as of January 2022.1 Given the divided national landscape and anecdotal evidence from our own patients, we hypothesized that low Covid-19 vaccination rates would be associated with decreases in influenza vaccination rates.
This polarization was a deliberate attempt by the Trump administration and his allies on the extreme right to politicise the pandemic, believing they would make political capital from such polarization. As things turned out, all they achieved was fooling their own supporters into risking serious illness and death from COVID-19, and now, as this article shows, from a seasonal flue epidemic.
The American Republican Pary is probably the first political party in history to promote policies that make their own supporters sick and take part in what some commentators have likened to a self-inflicted genocide of right-wing covidiot Trumpanzees, and Trumpanzee cultists are probably the first political faction who think policies which seem designed to harm them, are good things to vote for.
Trends in age adjusted mortality rates (AAMRs) per 100 000 population of residents of counties voting for Democratic or Republican presidential candidates by urban-rural location. Widening gaps in AAMR between Republican and Democratic counties are noted across urban-rural spectrum, from large metropolitan areas, medium metropolitan areas, and rural areas
…found what they call a “mortality gap” — a widening difference between age-adjusted death rates in counties that had voted for a Democrat or a Republican in previous presidential and governor elections. The team found that mortality rates decreased by 22 percent in Democratic counties but by only 11 percent in Republican counties. The mortality gap rose across top disease areas, including heart disease and cancer, and the mortality gap between white residents in Democratic versus Republican counties increased nearly fourfold during the study period.
The press release goes on to say:
In an ideal world, politics and health would be independent of each other and it wouldn’t matter whether one lives in an area that voted for one party or another, but that is no longer the case. From our data, we can see that the risk of premature death is higher for people living in a county that voted Republican.
Our study suggests that the mortality gap is a modern phenomenon, not an inevitability. At the start of our study, we saw little difference in mortality rates in Democratic and Republican counties. We hope that our findings will open people’s eyes and show the real effect that politics and health policy can have on people’s lives.
Assistant professor Haider Warraich, MD, lead author
Division of Cardiovascular Medicine
Brigham and Women’s Hospital, Boston, MA, USA
Warraich and colleagues used data from the Wide-ranging OnLine Data for Epidemiologic Research (CDC WONDER) database and the MIT (Massachusetts Institute of Technology) Election Data and Science Laboratory. They classified counties as Democratic or Republican based on the way the county had voted in the previous presidential election and adjusted for age when calculating mortality rates.
Overall, the team found that mortality rates in Democratic counties dropped from 850 deaths per 100,000 people to 664 (22 percent), but in Republican counties, mortality rates declined from 867 to 771 (11 percent). When the team analyzed by race, they found that there was little gap between the improvements in mortality rates that Black and Hispanic Americans experienced in Democratic and Republican counties. But among white Americans, the gap between people living in Democratic versus Republican counties was substantial.
The mortality gap remained consistent when the researchers looked only at counties that had voted Republican or Democratic in every presidential election year studied and when they looked at gubernatorial elections. Democratic counties experienced greater reductions in mortality rates across most common causes of death, including heart disease, cancer, chronic lower respiratory tract diseases, diabetes, influenza and pneumonia, and kidney disease.
The authors note that the widening gap in death rates may reflect the influence of politics on health policies. One of the inflection points detected in the study corresponds to the Affordable Care Act (ACA), which was passed in 2010. More Democratic states than Republican states adopted Medicaid expansion under the ACA, which expanded health insurance coverage to people on a low income.
The study detects an association between political environment and mortality but does not definitively determine the direction of the association or the specific factors that may explain the link between the two. The authors did not study the effect of flipping political environments — that is, counties that switched from voting Democratic or Republican to voting for the other party — on health outcomes, which could be an area of future study. The study period ended in 2019, before the start of the COVID-19 pandemic, which may have had an even more profound impact on the mortality gap.
Trends in age adjusted mortality rates (AAMRs) per 100 000 residents of counties voting for Democratic or Republican presidential candidates. Widening gap in AAMR is noted between Democratic and Republican counties. Statistically significant inflection points in annual percentage change (APC) of AAMR occurred for Democratic counties between periods 2001-09 (APC −2.1) and 2009-19 (APC −0.8) and Republican counties between periods 2001-08 (APC −1.4) and 2008-19 (APC −0.2)
Trends in age adjusted mortality rates (AAMRs) per 100 000 residents of counties voting for Democratic or Republican presidential candidates by sex. Widening gap in AAMR is noted between male and female residents of Democratic and Republican counties. (Top lines) Statistically significant inflection points in annual percentage change (APC) of AAMR occurred for male residents of Democratic counties between periods 2001-10 (APC −2.2) and 2010-19 (APC −0.7) and male residents of Republican counties between periods 2001-07 (APC −1.7) and 2007-14 (APC −0.6) with no significant change noted after additional inflection point (straight line) between 2014 and 2019. (Bottom lines) Statistically significant inflection points in annual percentage change of AAMR occurred for female residents of Democratic counties between periods 2001-09 (APC −2.0) and 2009-19 (APC −0.9) and female residents of Republican counties between periods 2001-07 (APC −1.4) and 2007-19 (APC −0.3).
Trends in age adjusted mortality rates (AAMRs) per 100 000 residents of counties voting for Democratic or Republican presidential candidates by race and ethnicity. Widening gap in AAMR is noted most prominently among white residents of Democratic and Republican counties, while the gap appears to narrow for Hispanic residents. AAMR gap for black residents of Democratic and Republican counties oscillates across the study period.
Trends in age adjusted mortality rates (AAMRs) per 100 000 population for counties voting for Democratic or Republican governors by state Group from 2001 to 2019. Group A=New Hampshire and Vermont; Group B=Alabama, Alaska, Arizona, Arkansas, California, Colorado, Connecticut, Florida, Georgia, Hawaii, Idaho, Illinois, Iowa, Kansas, Maine, Maryland, Massachusetts, Michigan, Minnesota, Nebraska, Nevada, New Mexico, New York, Ohio, Oklahoma, Oregon, Pennsylvania, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Wisconsin, Wyoming, and Washington DC; Group C=Delaware, Indiana, Missouri, Montana, North Carolina, North Dakota, Utah, Washington, and West Virginia; Group D=Kentucky, Louisiana, and Mississippi; Group E=New Jersey and Virginia.
Trends in age adjusted mortality rates (AAMRs) per 100 000 population of residents of counties voting for Democratic or Republican presidential candidates by urban-rural location. Widening gaps in AAMR between Republican and Democratic counties are noted across urban-rural spectrum, from large metropolitan areas, medium metropolitan areas, and rural areas.
Age adjusted mortality rates (AAMRs) per 100 000 population for the 10 most common causes of death in Democratic and Republican counties in 2001 and 2019. Except for cerebrovascular disease, the gap in AAMR between Republican and Democratic counties increased for every cause of death over the study period driven by heart disease, cancer, chronic lower respiratory tract disease, unintentional injuries (which include drug overdoses), and suicide.
As these charts show, this gap holds true for all demographic grouping, whether by sex, race, geography or age and even for the 10 most common causes of death. However the biggest gap is seen in the white population. This is significant because the Republican Party is increasingly becoming identified as the party of the white right.
On every measure, Americans living in red counties fare worse that those living in blue counties and the authors point out the study period ended in 2019 before the COVID-19 pandemic. They also point out that one of the inflections on the charts during which the health of those in Democrat counties improved more than the health of those in Republican counties coincided with President Obama's, Affordable Care Act, which was implemented disproportionately in Democrat counties and improved the health of poor people.
As these figures show, the Republicans who campaigned against 'Obama Care' were in effect campaigning against improving the health of their own supporters!
It will be interesting to see what happened during the later stages of the COVID-19 pandemic after vaccinations against the virus had become widely available, and especially during the omicron variant wave, when most Democrat voters had been vaccinated and were observing sensible precautions, and, following the disastrously incompetent lead of Donald Trump and his allies on the extreme political right, and in the white supremacist evangelical Christian churches, many covidiot Republicans failed to get vaccinated and refused to wear face-coverings or observe social distancing because they had all become seen as anti-Trump statements!
This deliberate division of American into partisan camps, for what Trump and his allies thought would be to their political advantage, resulted in hospital admissions and deaths from COVID-19 being disproportionately of Republican antivaxxer covidiots in what some commentators likened to a self-inflicted genocide of fundamentalist, covidiot Trumpanzees. Probably the first time in the history of democracy that a political party has actively pursued policies that seem designed to kill their own supporters and their supporters trotted dutifully along like lambs to the slaughter led by Judas sheep, and yet only a tiny handful of Republican politicians had the decency to back out of the rabbit hole they had dived into and take the poitical risk of admitting they were wrong.
The teams finding are published, open access, in the BMJ:
Abstract
Objective To assess recent trends in age adjusted mortality rates (AAMRs) in the United States based on county level presidential voting patterns.
Design Cross sectional study.
Setting USA, 2001-19.
Participants 99.8% of the US population.
Main outcome measures AAMR per 100 000 population and average annual percentage change (APC).
Methods The Centers for Disease Control and Prevention WONDER database was linked to county level data on US presidential elections. County political environment was classified as either Democratic or Republican for the four years that followed a November presidential election. Additional sensitivity analyses analyzed AAMR trends for counties that voted only for one party throughout the study, and county level gubernatorial election results and state level AAMR trends. Joinpoint analysis was used to assess for an inflection point in APC trends.
Results The study period covered five presidential elections from 2000 to 2019. From 2001 to 2019, the AAMR per 100 000 population decreased by 22% in Democratic counties, from 850.3 to 664.0 (average APC −1.4%, 95% confidence interval −1.5% to −1.2%), but by only 11% in Republican counties, from 867.0 to 771.1 (average APC −0.7%, −0.9% to −0.5%). The gap in AAMR between Democratic and Republican counties therefore widened from 16.7 (95% confidence interval 16.6 to 16.8) to 107.1 (106.5 to 107.7). Statistically significant inflection points in APC occurred for Democratic counties between periods 2001-09 (APC −2.1%, −2.3% to −1.9%) and 2009-19 (APC −0.8%, −1.0% to −0.6%). For Republican counties between 2001 and 2008 the APC was −1.4% (−1.8% to −1.0%), slowing to near zero between 2008 and 2019 (APC −0.2%, −0.4% to 0.0%). Male and female residents of Democratic counties experienced both lower AAMR and twice the relative decrease in AAMR than did those in Republican counties. Black Americans experienced largely similar improvement in AAMR in both Democratic and Republican counties. However, the AAMR gap between white residents in Democratic versus Republican counties increased fourfold, from 24.7 (95% confidence interval 24.6 to 24.8) to 101.3 (101.0 to 101.6). Rural Republican counties experienced the highest AAMR and the least improvement. All trends were similar when comparing counties that did not switch political environment throughout the period and when gubernatorial election results were used. The greatest contributors to the widening AAMR gap between Republican and Democratic counties were heart disease (difference in AAMRs 27.6), cancer (17.3), and chronic lower respiratory tract diseases (8.3), followed by unintentional injuries (3.3) and suicide (3.0).
Conclusion The mortality gap in Republican voting counties compared with Democratic voting counties has grown over time, especially for white populations, and that gap began to widen after 2008.
I would suggest to my American readers in particular, that a party which is actively and knowingly pursuing policies designed to make their people sicker with a lower life expectancy, is a party which should never be trusted with the power to implement those policies at any level of government.
New research shows that, although unvaccinated children produce antibodies and killer T-cells in response to COVID-19 infection, this response may not be strong enough to protect them against future variants, especially if the antibodies fail to recognise the variant.
The normal response to viral infections is two-fold. First there are the antibodies that are produced in response to the foreign proteins. These bind to the viruses, deactivate them and cause them to clump together so they can be moped up by phagocytic white cells. However, they can only act against circulating viruses and not against viruses that have already gained access to the cells, where they will be replicating.
The second response is the more long-term one. This produces pre-programmed killer T-lymphocytes or 'memory' T-cells - white blood cells - that recognise infected cells and destroy them, together with the viruses inside them, to prevent them infecting other cells or being shed to infect other people, so limiting the infection and minimising the damage to the infected tissues. T-cells can provide protection even when the antibodies fail to recognise the virus because they are produced in response to stable fragments of viral proteins that are less likely to differ in different variants, hence they safeguard against future mutant forms.
Neither of these is 100% effective of course and people can still become infected again and can still be infectious by shedding more viruses into the environment, but they do greatly reduce the seriousness of the infection and the risk of passing it on to other people.
However, what the researchers at the Doherty Institute, Melbourne, Australia, have shown is that unvaccinated children produce far fewer killer T-cells than adults. The researchers say this limited ability of unvaccinated children to generate strong memory killer T cell responses following natural infection may leave them vulnerable to future infections. The anti-COVID vaccines, on the other hand, are specifically designed to produce a strong T-cell response in addition to antibodies, placing vaccinated children as a significant advantage.
This study provides more evidence that Covid vaccination is safe for both current and future pregnancies, and shows in a mouse model that immunization during the earliest stages of pregnancy provides antiviral antibodies to the fetus throughout the rest of pregnancy.
Two of the bogus antivaxxer claims with which the politically-motivated covidiot antivaxxer movement is trying to scare women into not getting vaccinated against COVID-19 are:
The vaccines cause birth defects if given during pregnancy.
The vaccines reduce fertility or cause sterility in women by producing antibodies against the protein syncytin-1, which in humans and related primates is involved in attaching the placenta during pregnancy.
Now both of these antivaxxer claims have been exposed as lies by Alice Lu-Culligan and her colleagues of the Yale School of Medicine, in a paper published open access today in PLOS Biology.
The second piece of disinformation was based on the fact that a small part of the SARS-CoV-2 spike protein that antibodies are produced against by the vaccines has a short sequence of amino acids that is also found in syncytin-1.
This is hardly surprising since syncytin-1 is the remnant of an ancient retrovirus that has been co-opted to aid in the attachment of the placenta in many primates. In fact, it's one of many pieces of evidence of common descent since it is present in all the old-world primates, but not in the new-world primates. The Wikipedia entry for syncytin-1 reads:
Syncytin-1 also known as enverin is a protein found in humans and other primates that is encoded by the ERVW-1gene (endogenous retrovirus group W envelope member 1). Syncytin-1 is a cell-cell fusion protein whose function is best characterized in placental development.[3][4] The placenta in turn aids in embryo attachment to the uterus and establishment of a nutrient supply.
The gene encoding this protein is an endogenous retroviral element that is the remnant of an ancient retroviral infection integrated into the primate germ line. In the case of syncytin-1 (which is found in humans, apes, and Old World but not New World monkeys), this integration likely occurred more than 25 million years ago.[5] Syncytin-1 is one of two known syncytin proteins expressed in catarrhini primates (the other being syncytin-2) and one of many viral genomes incorporated on multiple occasions over evolutionary time in diverse mammalian species.[6]
ERVW-1 is located within ERVWE1,[7][8] a full length provirus on chromosome 7 at locus 7q21.2 flanked by long terminal repeats (LTRs) and is preceded by ERVW1 gag (Group AntiGen) and pol (POLymerase) within the provirus, both of which contain nonsense mutations rendering them non-coding.[9][10]
Syncytin-1 is also implicated in a number of neurological pathologies, most notably, multiple sclerosis, as an immunogen.
According to information made available ahead of publication by PLOS, Lu-Culligan and her colleagues:
A new study by Lude Franke and colleagues of the University of Groningen, Netherlands has shown that some individuals were more affected than others by the COVID-19 pandemic, due to their genes.
Of course, any omniscient designer of those genes and of the SARS-CoV-2 virus, such as the one intelligent [sic] design creationists believe is the creator of everything, will have been fully aware of that fact when it created the virus, so can't escape the charge of deliberately targeting certain individuals because of their genetics.
The difference is to be found in how well or badly individuals coped not so much with infection by the virus, but with the overall social effect of the pandemic, including the measures to mitigate and control it.
Even as the structure of SARS-CoV-2 changes with different variants of the virus (gray), the J08 antibody (blue) can still bind it, Scripps researchers showed.
Creationism’s beloved malevolence is going to have its work cut out it it is to outdo bio-medical science in their search for a definitive cure for the COVID-19 virus it created to cause the current COVID-19 Pandemic. So far, it has come up with several variants, the latest being the Omicron variant that is much more contagious than earlier variants, but, at least in a population where a large proportion of the people have been vaccinated, is mostly, though not always, a relatively mild infection.
Nevertheless, it has managed to achieve nearly 6.3 million deaths worldwide, 1 million of them in the USA where, due to the incompetence and narcissistic Dunning-Kruger stupidity of the president when the pandemic started and was most dangerous in 2020, and because of the opposition to measures to control it by fundamentalist Christians and the super spreader events they insisted on holding in their churches, deaths were far in excess of anything seen in most other advanced economies.
But now, a collaborative effort between scientists at the Scripps Institute and scientists in Italy and France may have found an antibody to the SARS-CoV-2 virus that not only treats and prevents known variants of COVID-19 but will probably be effective against future variants. The antibody is currently undergoing stage II/III clinical trials in Italy. The antibody, known as J08 was isolated from the blood of people who had recovered from COVID19 by scientists at the Scripps Institute and Toscana Life Sciences.
The question creationist devotees of the magic, pestilential sky man whom they believe designs these things, is just how is it going to find a way round this new prevention/treatment so it can continue the chaos and suffering it created? Only time will tell.